
Acute Multiple Sclerosis Exacerbation: A Quick Overview
Although the precise cause of MS remains unclear, current evidence suggests that the disease develops when genetically susceptible individuals encounter environmental triggers that initiate immune-mediated damage within the central nervous system

As the most common CNS autoimmune disease in the world, Multiple Sclerosis (MS) is well known, but not well understood. Currently, MS is categorized into differing subtypes, including: relapsing and remitting MS (RRMS), primary progressive MS (PPMS), secondary progressive MS (SPMS), and clinically isolated syndrome (CIS), among others. RRMS is the most common form, constituting roughly 80-85% of diagnoses and being distinguishable through acute exacerbation episodes/relapses separated by periods of "stable" disease.
Background:1,2
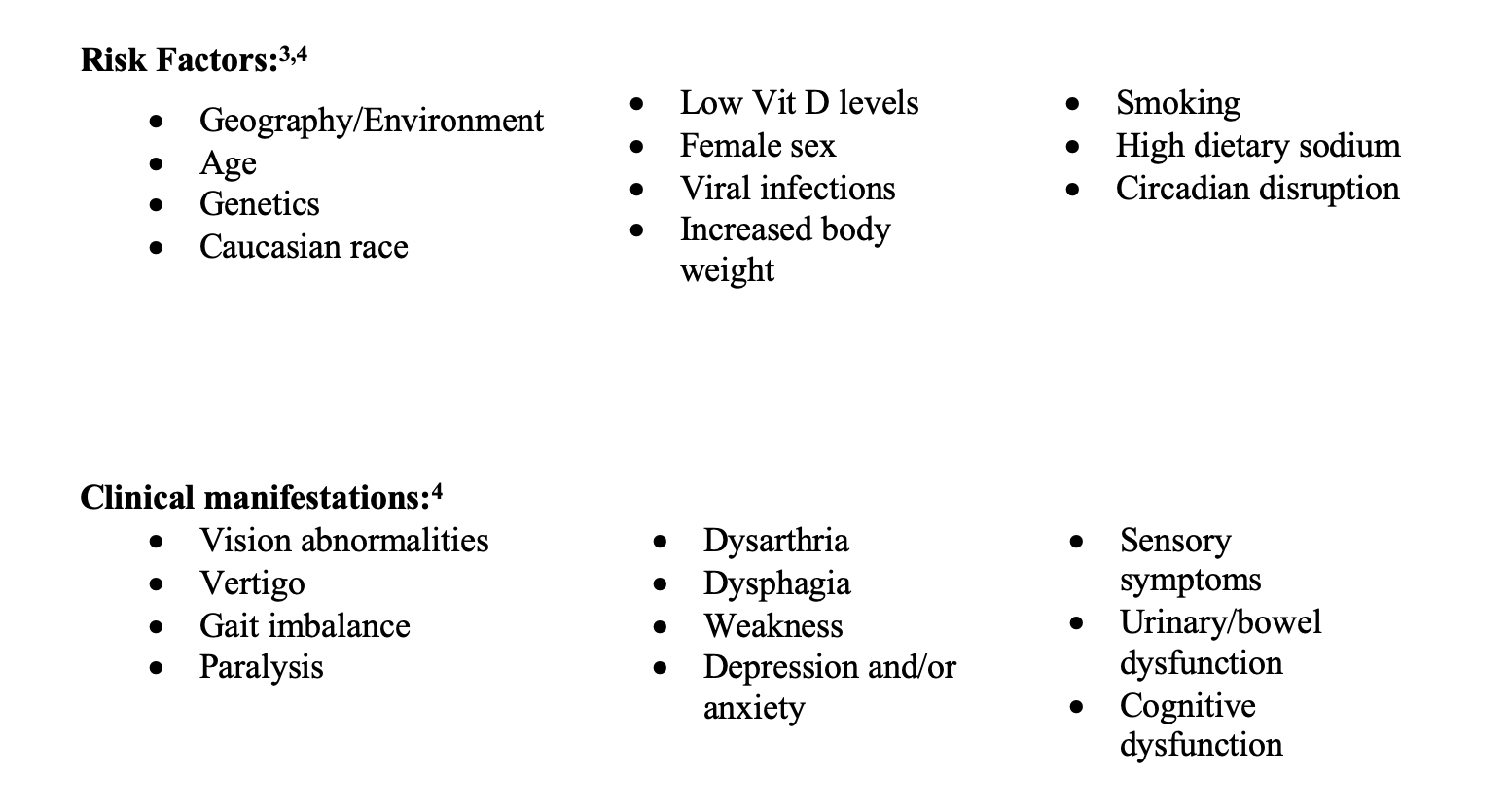
Multiple Sclerosis (MS) affects roughly 2.8 million people worldwide (35.9/100,000 population). The average age of diagnosis ranges from 20 to 40 years and affects females more commonly than males at a ratio of 3:1. The disease is more common farther from the equator, thought to be due to differences in sunlight exposure and vitamin D levels, in part due to immunomodulatory effects of Vitamin D. Additional components of the disease include a history of Epstein-Barr virus infections (most people in the world), which on its own may not cause MS, but can be a driver/trigger in those with a genetic predisposition.
Pathophysiology:3,4
Although the precise cause of MS remains unclear, current evidence suggests that the disease develops when genetically susceptible individuals encounter environmental triggers that initiate immune-mediated damage within the central nervous system. Leading origins of disease include:
1. Neurodegenerative processes leading to the release of antigenic constituents from the central nervous system to the periphery, where immune cells may become sensitised and primed for future self-aimed destruction.
2. Immune cell infiltration of the central nervous system through the blood-brain barrier, subarachnoid space, or choroid plexus across the blood-cerebrospinal fluid barrier.
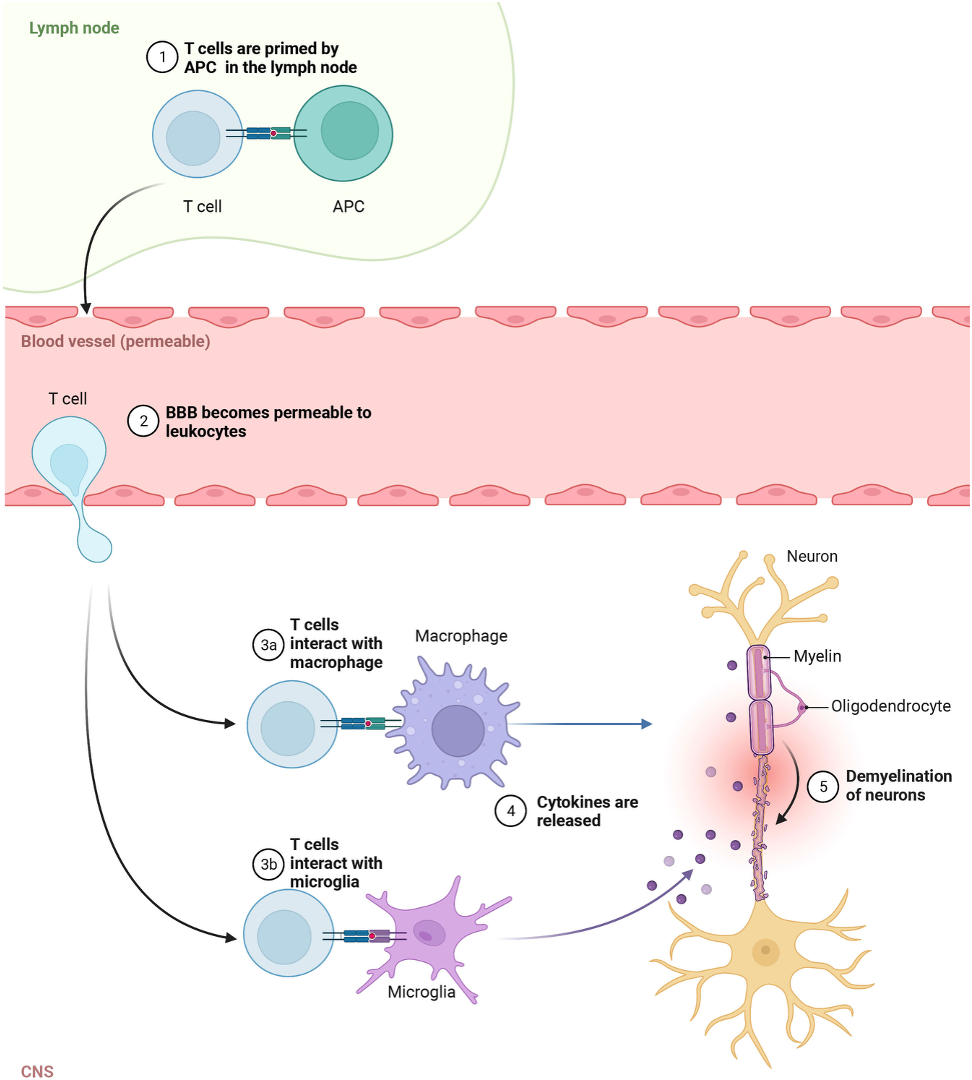
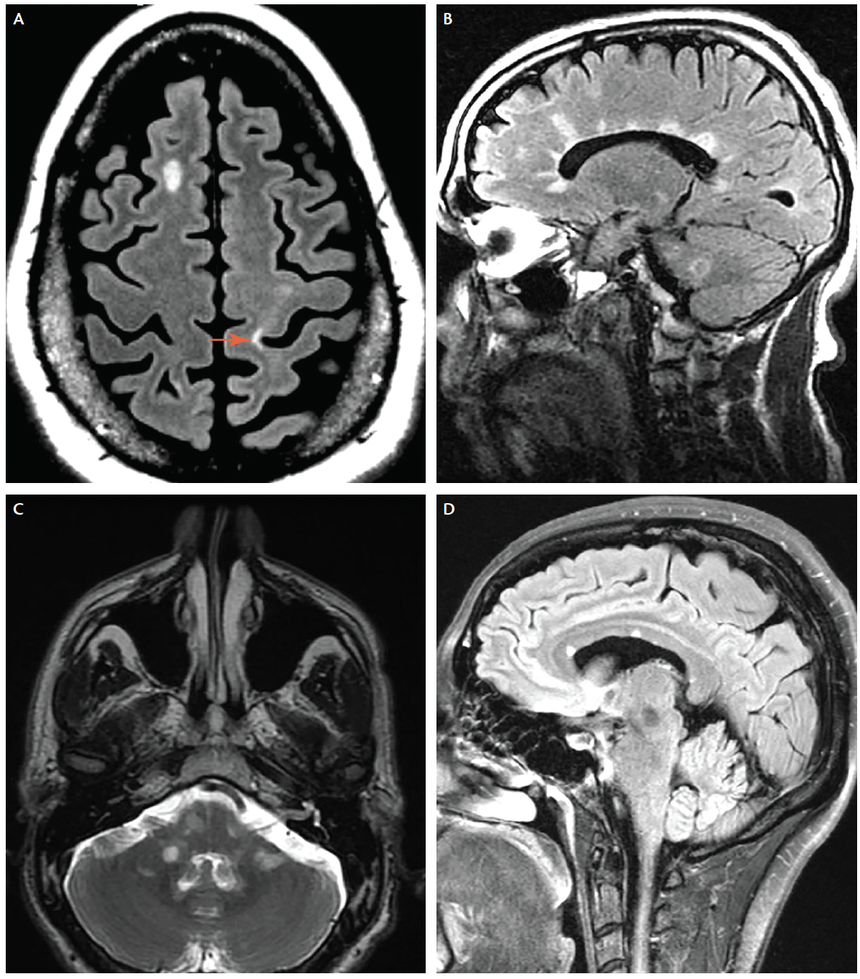
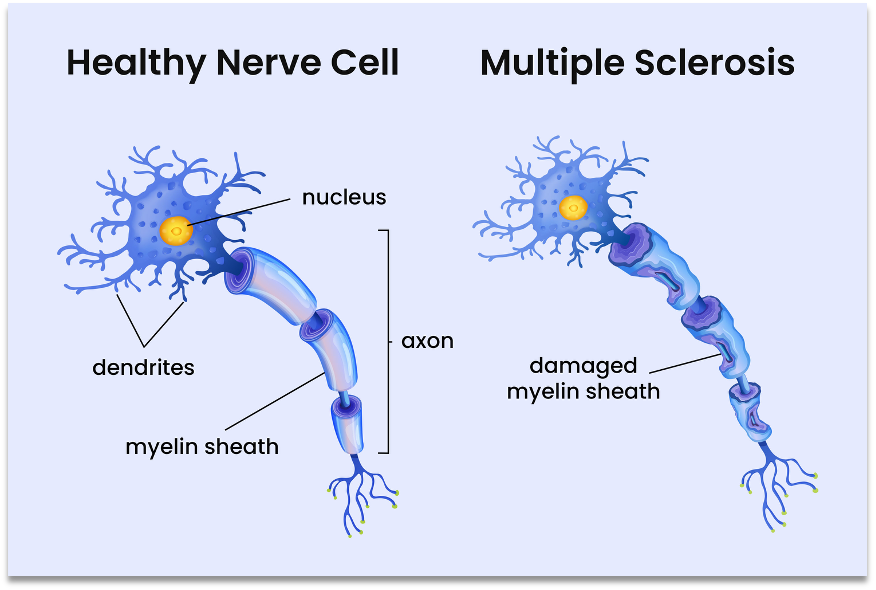
Regardless of origins, autoreactive immune cells target myelin basic protein and degrade myelin. This includes T/B cells, macrophages, and complement. Demyelination increases axonal susceptibility to damage, which is irreversible if severed. Ultimately, the two fundamental underlying processes in disease include focal inflammation, visible as macroscopic plaques, as well as neurodegeneration of the CNS.
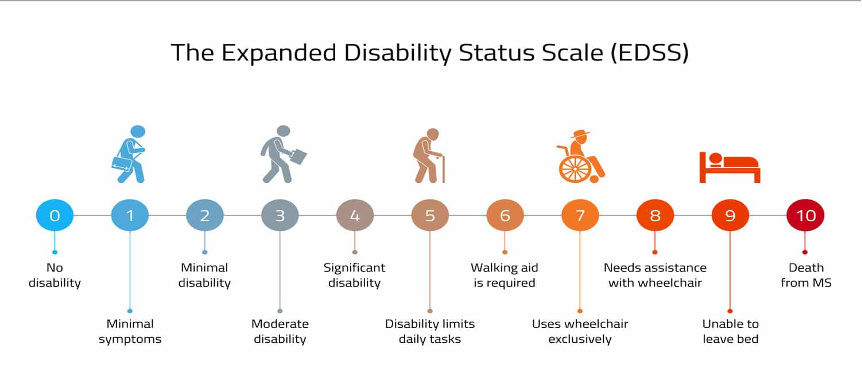
Disability scoring tools:5
The Expanded Disability Status Scale (EDSS): A 0-10 scale predominantly assessed by neurologists to quantify disability based on clinical examinations. It measures impairment across eight functional systems and is rated by the severity and number of functional systems impacted, as well as ambulatory ability. The eight functional systems include: pyramidal, cerebellar, brainstem, sensory, bowel and bladder, visual, cerebral, and "other". Feel free to peruse the MDCALC tool here!
Relapsing-remitting course:4
Characterised by relapses of neurologic symptoms with stability between, new or recurrent symptoms develop over days to weeks and can present vastly differently for each individual - consider that different neural pathways and areas of the brain may be affected (not everyone will have an MS lesion at the same location in the CNS). This is why the EDSS scale takes into account the differing functional systems. Evaluation is reliant on patient history and physical examination, MRI findings, CSF or blood studies, as well as excluding other causes of the patient's symptoms. The diagnosis of an acute exacerbation/relapse is supported by evidence of historical relapses, confirmed through evidence of one or more lesions.
Treatment:4
Addressing underlying triggers for a relapse, such as infection, heat, stress, or metabolic derangement, should be the primary focus to hopefully mitigate subsequent relapses.
With new onset or acutely worsening neurologic symptoms leading to increased disability, you may consider the following treatment strategies to improve recovery time:
- High-Dose Corticosteroids - two common options include:
- 500 to 1,000 mg IV methylprednisolone for 3 to 7 days, optionally followed by a short prednisone taper.
- 1,250 mg prednisone daily for 3 to 7 days, with or without a short taper (this is an alternative to 1,000 mg oral methylprednisolone daily)
Monitoring for corticosteroids includes mood alterations such as agitation/depression (consider PHQ-9 assessments), insomnia, hyperglycemia, leukocytosis, fluid retention, GI upset, and signs and symptoms of bleeding, among others.
Later lines of therapy:
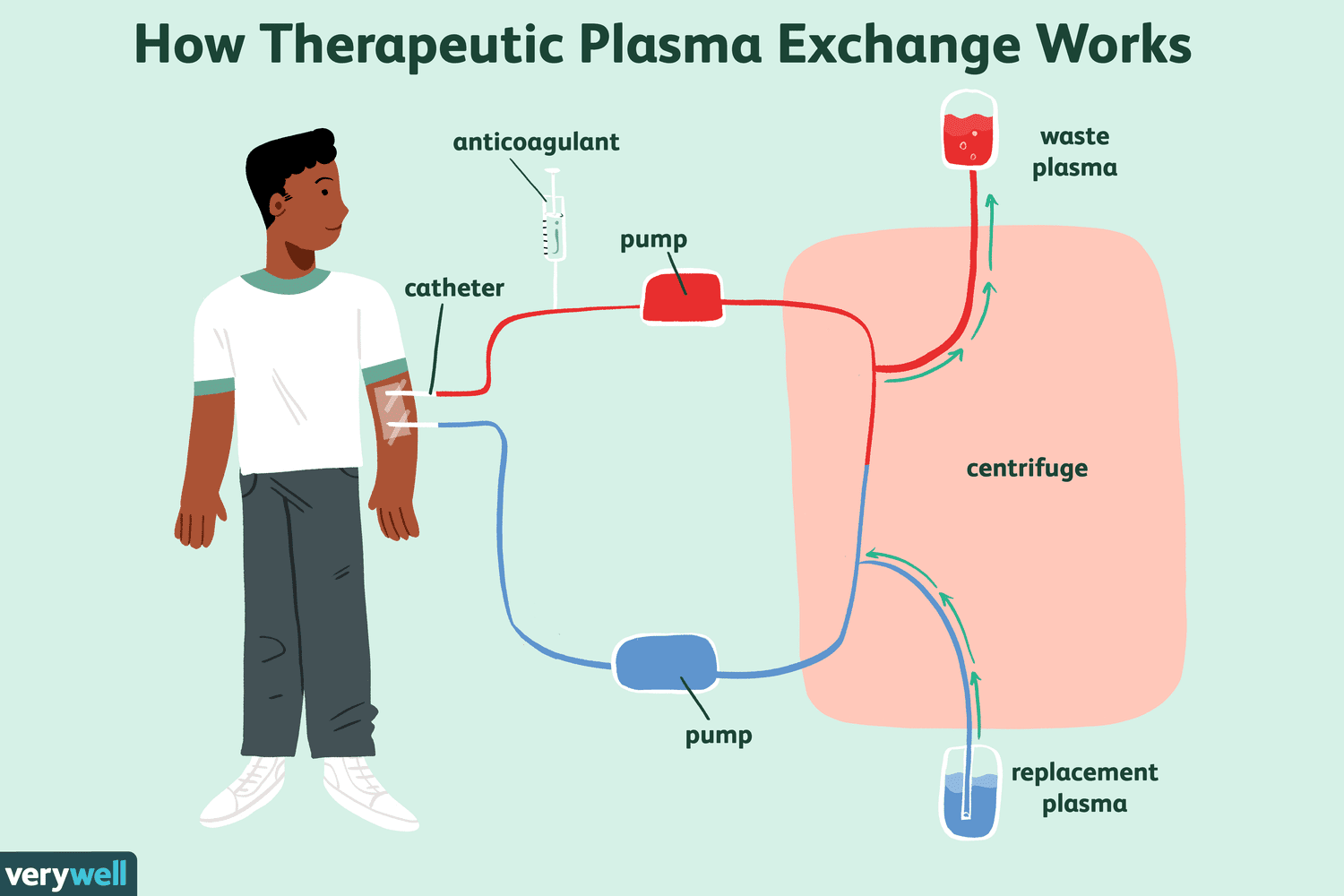
- Plasma exchange every day or every other day for a total of 3 to 7 treatments is an option in those resistant to corticosteroid treatment.
- Monitor for fever, chills, urticaria, muscle cramps, hypotension, dizziness, bleeding, infections, and allergic reactions
- IVIG 0.4g/kg/day over 5 days given as a continuous infusion, is often considered a 3rd line option
- Monitor for headaches, fever, chills, fatigue, dizziness, nausea, thrombosis, renal dysfunction/acute renal failure, bleeding, infections, allergic reactions
Bonus info:
Consider a short course of gastroprotective agents such as H2RAs or PPIs to avoid GI bleeding with our corticosteroid medications. Corticosteroids inhibit the synthesis of prostaglandins, which help to produce the gastric mucosal protective barrier. It should be noted that this effect is present regardless of the route of administration (IV or Oral).
When possible, corticosteroids should be given earlier in the day to minimise insomnia risk. Prophylactic melatonin could be beneficial. There is some data to suggest oral steroids have a higher risk of insomnia, with some rationale being delayed bioavailability/onset given the additional absorption step required of oral medications. Here is a non-inferiority trial that showcased that oral methylprednisolone is non-inferior to IV regarding treatment efficacy but with higher rates of insomnia.
An additional survey study showed patient preference for oral corticosteroids over IV here.
*Information presented on RxTeach does not represent the opinion of any specific company, organization, or team other than the authors themselves. No patient-provider relationship is created.
References:
1. Portaccio E, Magyari M, Havrdova EK, et al. Multiple sclerosis: emerging epidemiological trends and redefining the clinical course. Lancet Reg Health Eur. 2024;44:100977. Published 2024 Aug 22. doi:10.1016/j.lanepe.2024.100977https://pmc.ncbi.nlm.nih.gov/articles/PMC7720355/
2. DiPiro J. DIPIRO’S PHARMACOTHERAPY : A Pathophysiologic Approach. Mcgraw-Hill Education; 2023.
3. Tafti D, Ehsan M, Xixis KL. Multiple Sclerosis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; March 20, 2024.https://www.ncbi.nlm.nih.gov/books/NBK499849/
4. Institute of Medicine (US) Committee on Multiple Sclerosis: Current Status and Strategies for the Future, Joy JE, Johnston RB Jr., eds. Multiple Sclerosis: Current Status and Strategies for the Future. Washington (DC): National Academies Press (US); 2001.https://www.edmus.org/en/dl/scales/edmus_fs.pdf
5. Le Page E, Veillard D, Laplaud DA, et al. Oral versus intravenous high-dose methylprednisolone for treatment of relapses in patients with multiple sclerosis (COPOUSEP): a randomised, controlled, double-blind, non-inferiority trial. Lancet. 2015;386(9997):974-981. doi:10.1016/S0140-6736(15)61137-0