
Exploring the Unknown: Cryptogenic Stroke
Strokes always have a source of origin and a cause, right? Wrong. Sometimes in medicine, there isn't an etiology. One example, cryptogenic stroke.



Author: Alex Poppen, PharmD
Editor: Kristen Lindauer, PharmD, BCPS
Stroke. Time is tissue. BEFAST. Thrombolytics. Thrombectomy. Brain damage. These are all key terms that run through my mind when I think or hear of "stroke." In the classroom setting (and in topic discussions on APPEs or PGY1 rotations), we learn about the etiology of strokes. The why did this occur? The where did this clot originate from?
Sometimes in medicine, there isn't an etiology. There isn't a known source of origination. We have one of our favorite guests, Alex Poppen, PharmD, here to share the first of a two part series on Cryptogenic Stroke. Buckle up, and let's dive into this mystery of a diagnosis!

What is a Stroke?
A stroke, medically known as a cerebrovascular accident (CVA), is a sudden and often serious medical condition that occurs when there is a disruption in the blood supply to a part of the brain. There are two main types of stroke.
Hemorrhagic Stroke: This type of stroke happens when a blood vessel in the brain ruptures or leaks, causing bleeding in or around the brain tissue. Hemorrhagic strokes can result from various causes, including high blood pressure, aneurysms (weakened blood vessel walls), or arteriovenous malformations (abnormal tangles of blood vessels). The bleeding can lead to increased pressure in the skull, which can damage brain cells.
The symptoms of a stroke can vary depending on the part of the brain affected, but common signs and symptoms include:
- Sudden numbness or weakness in the face, arm, or leg, especially on one side of the body.
- Sudden confusion, trouble speaking, or difficulty understanding speech.
- Sudden trouble with vision in one or both eyes.
- Sudden severe headache with no known cause.
- Sudden dizziness, loss of balance, or lack of coordination.

Stroke is a medical emergency, and prompt treatment is crucial. The most effective treatment for ischemic strokes is to restore blood flow to the brain as quickly as possible, often through the use of a clot-busting medication called tissue plasminogen activator (tPA) or mechanical clot removal procedures. Hemorrhagic strokes may require surgical intervention to repair the bleeding blood vessel.
Stroke can have serious and lasting effects, including paralysis, cognitive impairment, and speech difficulties. Rehabilitation (e.g., speech, occupational, physical) is essential for stroke survivors to regain as much functionality as possible, and medical management (e.g., pharmacotherapy) is key for minimizing the potential for future strokes.
Types of Ischemic Stroke
The two main types of stroke are ischemic and hemorrhagic.
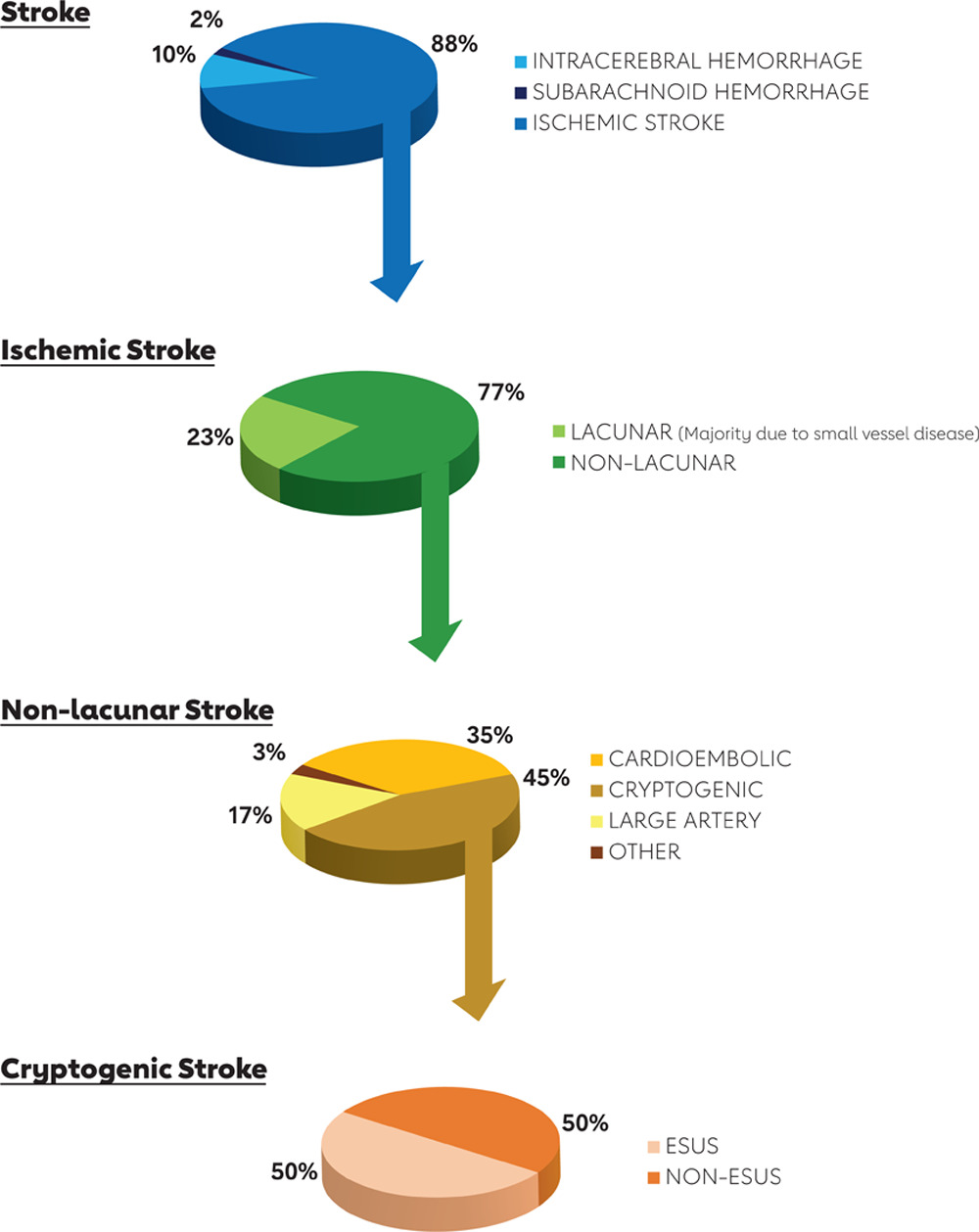
Ischemic is the most common type of stroke, accounting for approximately 85% of all strokes. Ischemic stroke can be further categorized as lacunar or non-lacunar.
Lacunar Stroke:
A lacunar stroke, also known as a lacunar infarct or lacunar syndrome, is a type of ischemic stroke that occurs when one of the brain's small, deep-seated arteries called "lenticulostriate arteries" or "penetrating arteries" become blocked or damaged.
Lacunar strokes are characterized by small, localized areas of brain damage. The term "lacunar" is derived from the Latin word for "hole" or "cavity," reflecting the small, well-defined nature of these infarcts.
The majority of lacunar strokes are due to small vessel disease.
Non-Lacunar Stroke:
A non-lacunar stroke, also known simply as an ischemic stroke, is a type of stroke that occurs when there is a blockage or obstruction in a larger, more central artery within the brain.
Non-lacunar strokes typically involve larger arteries that supply blood to more extensive areas of the brain. These arteries include the middle cerebral artery, anterior cerebral artery, posterior cerebral artery, and others.
Non-lacunar strokes often result in larger areas of brain tissue damage compared to lacunar strokes. The extent and location of the damage can vary, leading to a wide range of symptoms and functional deficits.
Non-lacunar (ischemic) strokes can be categorized into several different types based on the underlying cause or mechanism. The main types of non-lacunar ischemic strokes include:
- Large Artery Atherosclerosis: This type of stroke is caused by the narrowing or blockage of a large artery in the brain due to the buildup of atherosclerotic plaques (atherosclerosis). It is often associated with risk factors such as high blood pressure, high cholesterol, and smoking.
- Cardioembolic Stroke: Cardioembolic strokes occur when a blood clot or debris, often originating in the heart (e.g., due to atrial fibrillation, heart valve disorders, or heart attacks), travels through the bloodstream and lodges in a brain artery, blocking blood flow.
- Cryptogenic Stroke: In cases where the cause of the stroke is unclear despite thorough evaluation, it may be classified as cryptogenic. This classification is often used when other potential causes have been ruled out.
These classifications are important for guiding treatment decisions and understanding the underlying mechanisms of the stroke. Determining the sub-type and cause of ischemic stroke helps healthcare providers tailor treatment plans and preventive measures to address the specific risk factors and causes associated with each subtype.
What is Cryptogenic Stroke?
- American Stroke Association (ASA) 2021 Secondary Prevention Guideline
Cryptogenic stroke (a type of ischemic stroke) can be further categorized into embolic stroke of undetermined source (ESUS) or non-embolic stroke of undetermined source (NON-ESUS).
Cryptogenic stroke is a diagnosis of exclusion.
Initial Work-Up
The minimum recommended evaluations for all patients suspected of ischemic stroke:
- Non-contrast brain CT or brain MRI to confirm the diagnosis of stroke
- Basic laboratory tests to gain insights into stroke risk factors
- Electrocardiogram to screen for atrial fibrillation, atrial flutter, and other cardiac conditions
Clarifying the underlying cause of cryptogenic stroke and identifying previously unrecognized risk factors has important implications for subsequent treatment and the risk of future strokes. Strategies for preventing secondary strokes should be customized based on the specific subtype of ischemic stroke.
Potential etiologies of cryptogenic stroke:
- Patent foramen ovale (PFO)
- Occult paroxysmal atrial fibrillation
- Hypercoagulable states
- Aortic arch atheroma
- Cardiac tumors
- Dissection
- Malignancy
- Vasculitis
Click on each section below for more information of the different etiologies!
Patent foramen ovale (PFO)
A patent foramen ovale (PFO) is a congenital heart condition where a small opening or flap in the heart's atrial septum, which usually closes shortly after birth, remains partially or completely open. This opening can allow blood to bypass the lungs and potentially carry small blood clots or debris from the venous circulation to the arterial circulation, increasing the risk of stroke and other cardiovascular issues. PFOs may require medical evaluation and, in some cases, closure procedures to reduce the risk of complications.
Assessment:
A bubble study, also known as a contrast study, is a diagnostic test used to assess the presence of a patent foramen ovale (PFO) in the heart. This test is typically performed during a transthoracic echocardiogram (TTE) or a transesophageal echocardiogram (TEE), both of which are types of ultrasound imaging of the heart.
A small amount of a contrast agent, usually tiny microbubbles within a saline solution, is injected into a vein in the patient's arm. If there is a PFO present, some of the microbubbles may pass from the right atrium to the left atrium of the heart through the open foramen ovale.
The choice between a TTE and TEE depends on factors such as the clinical suspicion of a PFO, the quality of images needed, and patient comfort. TEE tends to provide clearer images but requires the insertion of the esophageal probe, while TTE is non-invasive but may not always offer the same level of detail.
Occult paroxysmal atrial fibrillation
Occult paroxysmal atrial fibrillation (AF) is a type of irregular heart rhythm that occurs intermittently without noticeable symptoms. It increases the risk of stroke and is often challenging to detect. Treatment involves stroke prevention measures and heart rhythm control if needed. Detection typically requires specific heart monitoring tests.
Extended-term monitoring can identify atrial fibrillation (AF) in as many as 30% of individuals who have experienced a cryptogenic stroke.
Assessment:
- Holter monitor (non-invasive, but large and bulky): typically worn for 7 days
- Telemetry device (non-invasive, smaller and easier to wear): typically worn for up to 30 days
- Implantable loop recorder (invasive, inserted under skin): typically used for 6-36 months
A significant number of patients with occult paroxysmal AF are identified after more than 30 days of monitoring. Consideration for anticoagulation therapy (instead of antiplatelet therapy) is warranted in patients with newly discovered AF (among other treatment approaches).
Hypercoagulable states
Hypercoagulable or thrombophilic conditions are genetic or acquired disorders that increase the likelihood of forming blood clots inappropriately. These conditions are characterized by deficiencies and mutations in natural anticoagulants.
Consulting a hematologist is warranted to assist with this assessment and interpretation of test results.
Aortic arch atheroma
Aortic arch atheroma refers to the buildup of fatty deposits (atherosclerosis) in the inner lining of the aortic arch, which is a curved portion of the aorta (the body's main artery). These deposits can narrow the artery and potentially lead to reduced blood flow to the brain and other organs. Aortic arch atheroma is associated with an increased risk of stroke and may require medical management to reduce the risk of complications.
Assessment:
Aortic arch atheroma is typically detected through imaging studies (e.g., TEE, TTE) that visualize the aorta and its inner lining. The choice of imaging method depends on various factors, including the patient's clinical presentation, the availability of equipment, and the expertise of healthcare providers. Detection of aortic arch atheroma is important because it can contribute to an increased risk of stroke and other cardiovascular events. Once identified, management and treatment strategies can be tailored to reduce the risk of complications.
Cardiac tumors
While primary cardiac tumors are rare, individuals with these tumors face a heightened risk of stroke. For patients diagnosed with a left-sided cardiac tumor after experiencing a stroke or transient ischemic attack (TIA), surgical removal of the tumor can be advantageous in lowering the chances of another stroke.
Detection and diagnosis of cardiac tumors require a multidisciplinary approach involving cardiologists, radiologists, and cardiac surgeons. The choice of diagnostic tests (e.g., TEE, TTE, MRI) depends on the individual patient's clinical presentation and the suspected type of cardiac tumor. Early detection and accurate diagnosis are crucial for planning appropriate treatment and improving patient outcomes.
Dissection
Dissections refer to small tears or damage in the inner layers of the arteries, particularly the carotid and vertebral arteries that supply blood to the brain. These tears can create a flap or clot within the artery, leading to reduced blood flow to the brain. If a clot or debris dislodges and travels to the brain, it can block smaller blood vessels, causing an ischemic stroke by depriving brain tissue of oxygen and nutrients.
Dissections of the extracranial carotid or vertebral arteries are a relatively infrequent cause of ischemic stroke. They can arise from either trauma or occur spontaneously and are more frequently observed in younger individuals.
Assessment:
The most common way to diagnose arterial dissections is through imaging studies, including (but not limited to) CT angiography (CTA), magnetic resonance angiography or angiogram.
The choice of diagnostic method depends on factors such as the patient's clinical presentation, the suspected location of the dissection, and the available imaging resources. Early detection and diagnosis of arterial dissections are crucial for prompt treatment to prevent complications, including the risk of stroke or further vascular damage.
Malignancy
Cancer patients face a heightened risk of stroke, with cancer as a concurrent condition observed in 10% of hospitalized individuals with ischemic stroke in the United States. There are several potential causes of ischemic stroke in these patients, including factors that promote blood clot formation.
Vasculitis
Vasculitis is a group of rare conditions characterized by inflammation of blood vessels, including arteries. Inflammation can weaken and damage blood vessel walls, leading to narrowing or blockage of the vessels. In some cases, vasculitis can cause blood clots to form within the inflamed vessels. When these clots block blood flow to the brain, they can lead to an ischemic stroke by depriving brain tissue of oxygen and nutrients. Vasculitis can affect various organs and tissues, including the brain, and may require specialized treatment to reduce inflammation and prevent complications like stroke.
Assessment:
The detection of vasculitis involves a combination of clinical assessments, imaging studies, and laboratory tests.
Conclusion
Cryptogenic stroke is a type of ischemic stroke with no clear cause; it is a diagnosis of exclusion.
It involves intensive work-up, imaging and specialist consults to attempt to identify the source of the event.
Determining the sub-type and cause of ischemic stroke helps healthcare providers tailor treatment plans and preventive measures to address the specific risk factors and causes associated with each subtype.
Secondary prevention strategies for cryptogenic stroke generally include similar recommendations for ischemic stroke (guideline-recommended pharmacotherapy, managing/avoiding comorbid conditions, practicing healthy lifestyle habits, maintaining a healthy weight, smoking/alcohol cessation, etc.) as well as recommendations targeting any specific findings in a case-by-case basis.
References
- American Stroke Association. Five Key Facts About Stroke. [Internet]. Available from: https://www.stroke.org/en/professionals/stroke-resource-library/prevention/five-key-facts-about-stroke.
- American Stroke Association. 2021 Updated Healthcare Professional Guide Understanding Diagnosis and Treatment of Cryptogenic Stroke. [Internet]. Available from: https://www.stroke.org/-/media/Stroke-Files/Cryptogenic-Professional-Resource-Files/Cryptogenic-Professional-Guide-ucm-477051.pdf.
- Leary MC, Caplan LR. Cardioembolic stroke: An update on etiology, diagnosis and management. Ann Indian Acad Neurol. 2008;11(Suppl 1):S52-S63.
- Wessels T, Röttger C, Jauss M, Kaps M, Traupe H, Stolz E. Identification of embolic stroke patterns by diffusion-weighted MRI in clinically defined lacunar stroke syndromes. Stroke. 2005;36(4):757-761. doi:10.1161/01.STR.0000158908.48022.d7
- Arboix A, Alió J. Cardioembolic stroke: clinical features, specific cardiac disorders and prognosis. Curr Cardiol Rev. 2010;6(3):150-161. doi:10.2174/157340310791658730
- Sharobeam A, Churilov L, Parsons M, Donnan GA, Davis SM, Yan B. Patterns of Infarction on MRI in Patients With Acute Ischemic Stroke and Cardio-Embolism: A Systematic Review and Meta-Analysis. Front Neurol. 2020;11:606521. Published 2020 Dec 8. doi:10.3389/fneur.2020.606521
Additional Resources:
*Information presented on RxTeach does not represent the opinion of any specific company, organization, or team other than the authors themselves. No patient-provider relationship is created.