
Does Being In Good Shape Actually Make You Live Longer?
We've all heard stories about someone who was in great shape but still experienced an untimely death. This happens often enough that many people start to ask, "Does being in good shape really make a difference?"


We've all heard stories about someone who was in great shape but still experienced an untimely death. This happens often enough that many people start to ask, "Does being in good shape really make a difference?" In this post, I'll make the case that yes, it does make a difference. However, fitness, like many other things, has diminishing returns.
The focus of this article will be a publication from Mandsager et al. in 2018. This retrospective cohort study included 122,007 patients with an average age of 53.4 years old. Patients were placed into 1 of 5 categories based on their fitness level (low, below average, above average, high, and elite). These categories were based on the patients' cardiorespiratory fitness (CRF), which was calculated during an exercise treadmill test. Each category corresponded with performance capabilities relative to others in the cohort: low (<25th percentile), below average (25th-49th percentile), above average (50th-74th percentile), high (75th-97.6th percentile), and elite (≥97.7th percentile). The primary outcome of this study was all-cause mortality.
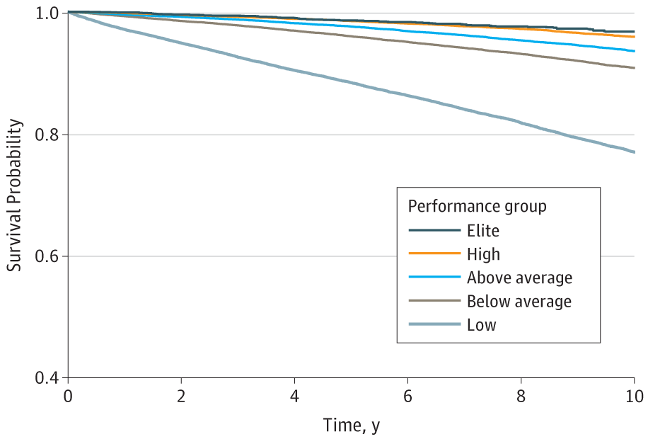
Above you'll see a graph showing the probability of survival over a 10 year period based on CRF in this cohort. Death from any cause occurred in 13,637 patients over a median follow-up of 8.4 years. The adjusted hazard ratio (aHR) for elite vs low performance groups was 0.20 (95% CI, 0.16-0.24; P < .001). In other words, elite performers were 5 times less likely to die from any cause over 10 years compared to the bottom 25% of performers.
You'll notice that there is not a huge difference between the high and elite performers (aHR = 1.29, hence diminishing returns), but there is a massive difference between the low and below average groups. The aHRs for low vs below average and low vs above average were 1.95 and 2.75 respectively (p < 0.001). That means the risk of dying was cut in half by going from a low to below average CRF. Even better, you'd be 2.75 times less likely to die if you went from a low to an above average CRF in this cohort. These are totally achievable goals, and the data suggests that they are absolutely worth pursuing! Even if you find yourself in the above average or high performance groups, there's still room to grow.
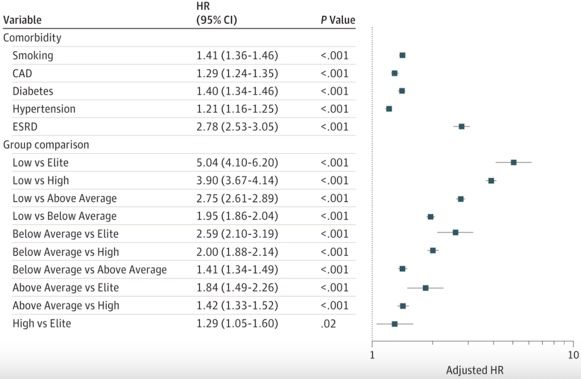
Above you'll see other striking findings from this cohort. For instance, there was a greater reduction in mortality risk by going from low to below average CRF than there was from not smoking, not having coronary artery disease, not having type-2 diabetes, or not having high blood pressure. The difference between low and above average performers was essentially equivalent to the risk associated with having end-stage renal disease!
Now, no study is perfect, and there are certainly some reservations to consider with this one. Firstly, this is a retrospective study (which does not prove causation) and is not as powerful as a prospective study or randomized control trial. You'll find this to be the case in similar studies as it's difficult to run a prospective trial with 8 years of follow-up. Additionally, it would be unethical to assign someone to a "no exercise group" and compare them to an "exercise group" for 10 years as all evidence would point to higher mortality risk in those not allowed to exercise. Similar ethical considerations are why you won't see a study prospectively evaluating a fast-food diet vs a whole foods diet over a decade. There are also some reservations around using the term "elite" to describe those scoring ≥97.7th percentile. It's likely that professional endurance athletes would actually have much better CRF scores than those in the "elite" group of this cohort, which might explain why other studies have shown U-shaped curves in cardiovascular risk for athletes (notably, many of those studies rely on self-reported fitness levels). Other issues include that this patient population consisted purely of those referred for an exercise treadmill test, and may not represent society at large. Additionally, there are likely several confounding variables that the investigators didn't adjust for such as socioeconomic class and ethnicity. Lastly, this study only utilized 1 exercise treadmill test per patient and therefore doesn't necessarily provide insight into the relationship between long-term fitness levels and mortality.
All this aside, this study supports the simple hypothesis that being in good shape actually makes you live longer, and I agree with the author's conclusions.