
How to "Prescribe" Exercise (Part 2): Aerobic Capacity
Part 2 of the series will kick off how to prescribe exercise to your patients, and we're starting with potentially the most important pillar of longevity: aerobic capacity.


Welcome back to part 2 of our new How to "Prescribe" Exercise Series! In our series introduction, we dove into some of the data on why we should prescribe exercise to our patients. If you haven't read that yet, consider going to our website and checking it out.
Part 2 of the series will kick off how to prescribe exercise to your patients, and we're starting with potentially the most important pillar of longevity: aerobic capacity. We've written on aerobic capacity before, so if you're a long-time reader of RxTeach, this next sentence won't surprise you. The focus of aerobic capacity training will be on 2 different aspects of the aerobic energy system: Zone 2 and VO2 max. Here is where I must assign your first bit of homework:
 Brentsen Wolf, PharmD
Brentsen Wolf, PharmD Brentsen Wolf, PharmD
Brentsen Wolf, PharmD
The first article on the benefits of Zone 2 training will take you through the basics of this energy zone, so please don't skip it! In order for you to properly understand how to prescribe exercise, you must have a deep understanding of Zone 2 and its benefits. For reference, here's a short bulleted list of some key points regarding Zone 2:
- To be in Zone 2, you have to maintain a heart rate that is 70-80% of your maximum
- Technical definition of Zone 2: Highest metabolic output you can sustain while keeping your lactate level below 2 mmol/L
- Zone 2 training optimizes fat oxidation as a fuel source
- In Zone 2, lactate levels are low, therefore increasing your ability to oxidize fat over carbohydrates
- The fitter you are, the higher "intensity related to peak power" you can maintain while still being in Zone 2
I hope that I've sufficiently stressed the importance of Zone 2 training and your understanding of it. Let's move on to VO2 max, which is at the other end of the spectrum for aerobic energy expenditure. Again, please read the article above! For reference, here's a short bulleted list of some key points regarding VO2 max:
- VO2 max is a measurement of how quickly you can utilize oxygen while exercising at max capacity
- Specifically, VO2 max measures how many mLs of oxygen you utilize per minute of exercise and is typically normalized by weight
- VO2 max is what most of the literature has used to show the association between fitness and longevity, of which there is overwhelming evidence

Prescribing Exercise
When prescribing exercise to your patients, you should make sure to target Zone 2 and VO2 max in order to optimize results and disease prevention. Hopefully you're starting with a motivated patient, but if not, I recommend taking Dr. Peter Attia's approach for explaining the necessity of training. Attia focuses on what he calls the "Centenarian Decathlon" in which he has his patients make a list of 10 activities they want to be able to do near the end of their lives. For example, this is Attia's list:
- Hike 1.5 miles on a hilly trail
- Get up off the floor under your own power, using a maximum of one arm for support
- Pick up a young child from the floor
- Carry two five-pound bags of groceries for five blocks
- Lift a twenty-pound suitcase into the overhead compartment of a plane
- Balance on one leg for thirty seconds, eyes open (Bonus points: eyes closed, fifteen seconds)
- Have sex
- Climb four flights of stairs in three minutes
- Open a jar
- Do thirty consecutive jump-rope skips
Attia then goes on to explain to his patients that it will be impossible for them to do many of these things in old age if they don't start training for it NOW. That's just the hard truth of aging, particularly aging without preparation. Aerobic capacity is essential to numbers 1, 4, 7, 8, and 10 on Attia's list. If your VO2 max is 30 mL/kg/min at age 40, you're setting yourself up for failure on all of these fronts. You will almost certainly not be able to do any of these things in your 90's, 80's, or even 70's without changing your approach. On the other hand, optimizing your approach will drastically increase your odds of doing these activities until the very end of your life. For reference, briskly walking up stairs requires a VO2 max of ~32. In order to quickly climb stairs at age 75, you would need a VO2 max of ~52 (or the ability to run a 1o minute mile on a 10% incline) at age 40, which is absolutely attainable for most people. Obviously, if you want to do more than quickly climb stairs at age 75, you'd need an even higher VO2 max in your 40s and 50s.
This is where your "prescription" comes in as a provider. Once you have an understanding of Zone 2 training as it pertains to heart rate monitoring and perceived effort, you can start to suggest training to your patients. Training in Zone 2 will increase your VO2 max. In fact, many patients who are not familiar with exercising should probably start here and worry about focused VO2 max training later. If your patient is starting from zero, any amount of added exercise will be beneficial. We know this from the Mandsager et al. publication which showed an all-cause mortality aHR for low vs. below-average cardiorespiratory fitness of 1.95 (p < 0.001). Just going from low to below-average fitness cuts your risk of dying from any cause in half.
Once you get past the initial benefits of starting to exercise, things get a little more challenging. In order to continue to gain value and increase your aerobic capacity, you should target at least 2 hours and 45 minutes of Zone 2 training per week. We've already exceeded the ADA recommendations with just one type of exercise. Depending on your patient's starting point, this time can be accrued doing any number of activities: hiking, biking, jogging, swimming, etc... Your patient should choose an activity that they enjoy if possible. They can always listen to music, podcasts, audiobooks, or even watch movies on a stationary bike if they choose. If you took Attia's approach to the Centenarian Decathlon, then you can suggest activities related to your patients' long-term goals.
Remember to explain to your patient how to tell if they're in Zone 2. As a reminder, there are 3 main ways of doing so:
- Measure lactate levels (common for elite athletes like professional cyclists and Olympic swimmers)
- Measure heart rate (common among athletes)
- Perceived exertion (easiest method)
Options 2 and 3 are by far the most common, and perceived effort requires no equipment. Explain to your patient that they should be able to speak in full sentences while exercising in Zone 2, but it should be difficult to do so.

More experienced athletes can start VO2 max training right away, and our other patients can join them after ~6 months of consistent Zone 2 training. As a reminder, VO2 max measures your maximum aerobic output. It also happens to be the measure with the most evidence to support an association with increased health-span. For that reason, you should absolutely encourage your patients to take a VO2 max test at least once per year so that they can track their progress.
See below for a table that tracks VO2 max by age, sex, and fitness level:
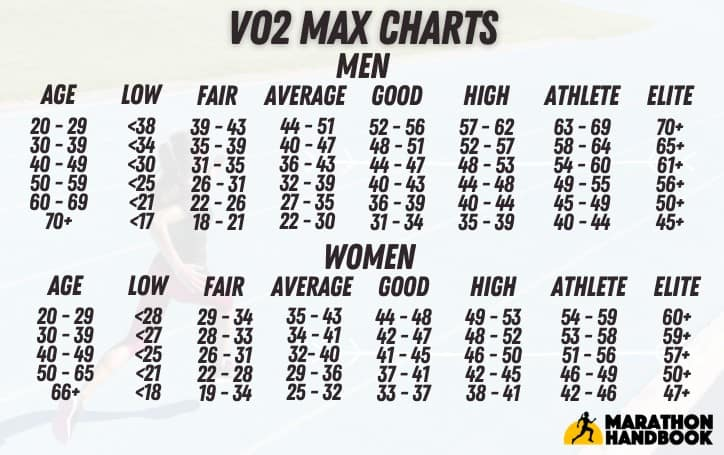
Progress will be very important in order for patients to actually meet their Centenarian Decathlon goals. According to Kim et al. in 2016, you can expect your V02 max to decline by 10-15% every decade. That's a hard pill to swallow. Without training, you will NOT be able to do the active things you enjoy later in life. The take home message here is that you can't afford to wait to start training, and neither can your patients.
As for prescribing VO2 max exercise to patients, it should be treated as a supplement. Your patients should not spend as much time training VO2 max as they do in Zone 2, unless they are training for very specific events. Patients should target 1-2 VO2 max training sessions per week. Again, we're now way beyond the ADA recommendations for time spent exercising. That's because we're interested in optimization here, not just getting by.
VO2 max training should be intense, but not an "all out" effort. Unlike HIIT cardio, VO2 max training should involve intervals that are at least 3 minutes long but that are unsustainable for more than 8-10 minutes. Patients can do the same activities for VO2 max as they do for Zone 2, but at a higher intensity. For example, you could advise your patient to try the following workout:
- 5-10 minute warm up
- 4 intervals of 4 minutes on and 4 minutes off (i.e. run hard for 4 minutes, then walk/jog for 4 minutes to recover, repeat x4)
- 5-10 minute cool down
That's an entire VO2 max workout in <45 minutes! The recovery period between sets should be long enough for your heart rate to drop back down to something just above a resting heart rate. You need to recover before going into your next working set. Your heart will actually get better and better at recovering between sets with training over time.
Look out on Wednesday, October 4th for the next article in this series where we will cover how to "prescribe" strength exercises for those interested in helping their patients live longer. Stay tuned.
*Information presented on RxTeach does not represent the opinion of any specific company, organization, or team other than the authors themselves. No patient-provider relationship is created.