
How Suzetrigine is Changing Pain Management
Read about how suzetrigine (Journavx) relieves acute pain without opioids through NaV1.8 inhibition, offering effective pain control safely.


For decades, the standard approach to treating severe acute pain meant flooding the central nervous system with opioid receptor agonists. We largely accepted that providing effective pain relief meant we also had to manage dangerous side effects like sedation, respiratory depression, and the risk of dependence. This reliance on opioid prescribing for moderate and severe pain has played a major role in fueling an overdose epidemic that still remains a public health crisis to this day.
The novel drug suzetrigine (Journavx) provides healthcare providers with a new way to approach acute pain. By shifting the focus away from the brain and toward the periphery, we now have an effective analgesic option for acute pain that completely bypasses the central nervous system.
How Suzetrigine Works
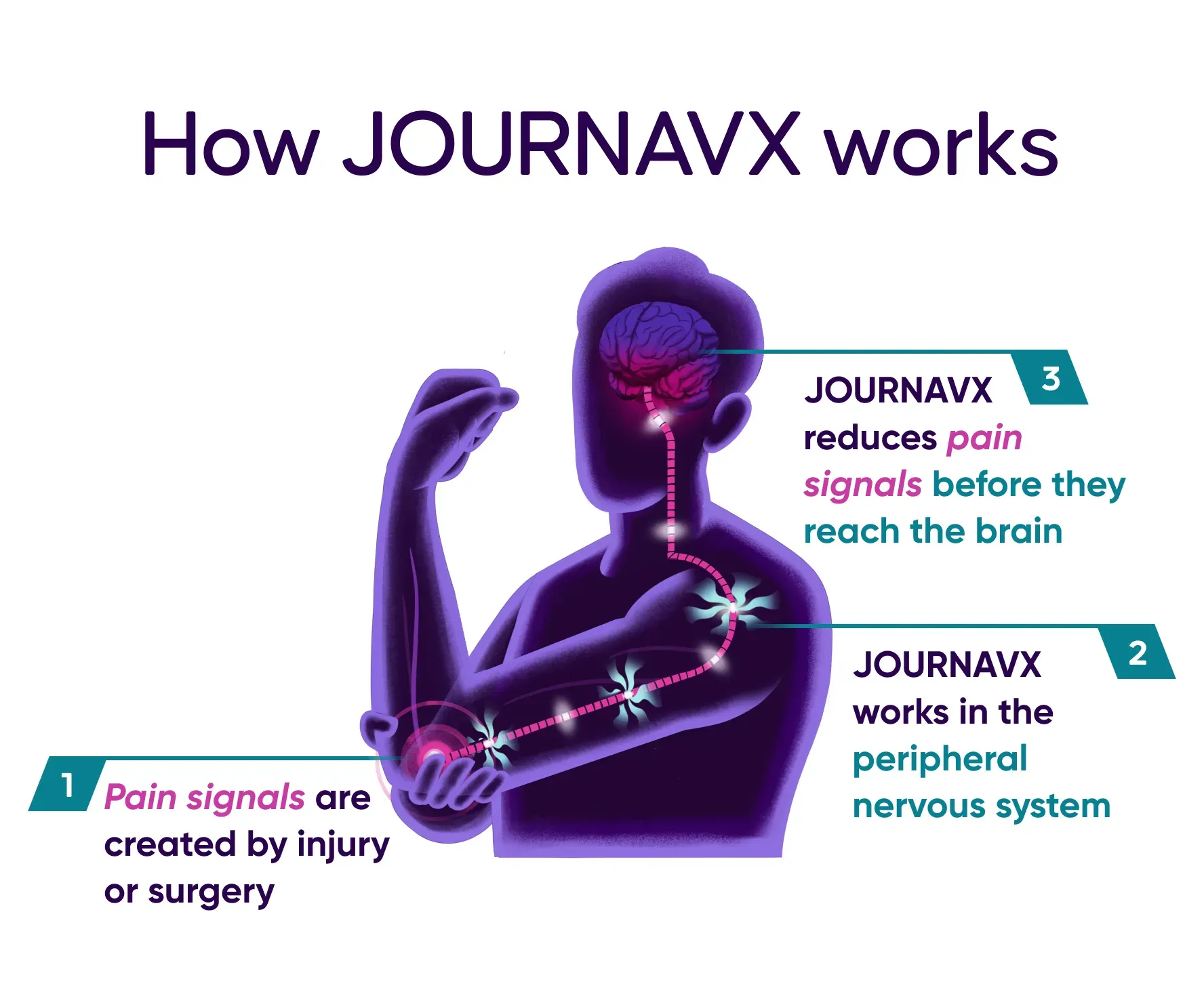
The pharmacology behind suzetrigine is distinctly different from that of opioids. Instead of masking the sensation of pain in the brain, suzetrigine stops the signal at the source. Suzetrigine works on NaV1.8 voltage-gated sodium channels, which are selectively expressed in peripheral nociceptive neurons. When our brains register the feeling of pain, it is because a nociceptor generated an action potential that was transmitted through our peripheral nervous system to our central nervous system.
Think of the NaV1.8 voltage-gated sodium channels in our peripheral nervous system like a series of active electrical wires. When tissue damage occurs, these specific wires send the action potential directly from the site of an injury up to the brain. Suzetrigine acts as a highly selective inhibitor of these NaV1.8 channels. Suzetrigine cuts the action potential off before it has a chance to make it to the central nervous system and register as the feeling of pain.
Clinical Evidence
The clinical data supporting suzetrigine demonstrate that it can hold its own compared to traditional opioid treatment. It provides a heavy-hitting, non-opioid alternative for patients needing serious relief.
- Bertoch et al. (2025): This study contained two Phase 3 randomized, double-blind, placebo- and active-controlled clinical trials evaluating suzetrigine's efficacy. The researchers investigated the drug in adults experiencing moderate-to-severe acute pain following either abdominoplasty or bunionectomy surgeries. Patients were randomized to receive suzetrigine, hydrocodone/acetaminophen, or placebo for 48 hours. The trials successfully achieved their primary endpoint, demonstrating that suzetrigine provided a statistically significant and clinically meaningful reduction in pain intensity over 48 hours compared to the placebo. While suzetrigine did not show superiority over hydrocodone/acetaminophen, it achieved similar levels of pain reduction as the hydrocodone/acetaminophen group.
- McCoun et al. (2025): To understand the utility of the drug outside of surgical environments, another Phase 3 single-arm study looked at broader applications for suzetrigine. The trial evaluated the safety and effectiveness of suzetrigine across a wide range of both surgical and non-surgical moderate-to-severe acute pain scenarios for up to 14 days. The primary endpoint was safety and the secondary endpoint was patient perception of pain control. The results were positive, with over 83% of the participants rating suzetrigine's effectiveness for treating their acute pain as good, very good, or excellent on a patient global assessment.
- ICER Review (2025): The Institute for Clinical and Economic Review comprehensively evaluated the drug for its overall clinical value. Their Midwest Comparative Effectiveness Public Advisory Council summarized that suzetrigine demonstrates clear effectiveness and value for patients dealing with moderate to severe acute pain.
Dosing and Considerations
The recommended starting dose of suzetrigine is a 100 mg loading dose, which consists of two 50 mg tablets. This initial dose must be taken on an empty stomach at least one hour before or two hours after food, although clear liquids are permitted. Beginning 12 hours after the loading dose, patients transition to a maintenance dose of one 50 mg tablet every 12 hours. These subsequent doses can be taken with or without food. Suzetrigine is intended for short-term use only and has not been studied for acute pain lasting beyond 14 days.
Dose reductions are required for patients with moderate hepatic impairment or those taking moderate CYP3A inhibitors. The medication is contraindicated in patients taking strong CYP3A inhibitors and should be avoided in severe hepatic impairment.
Notable reported adverse effects of suzetrigine are skin rash, muscle spasm, increased creatinine phosphokinase in blood, and decreased eGFR (estimated glomerular filtration rate – a measure of kidney function).
Conclusion
Suzetrigine is not just another alternative pain medication on the formulary. Suzetrigine is a novel drug with a completely new mechanism of action that changes the way we can approach moderate and severe pain. By utilizing peripheral NaV1.8 nerve blockers, pharmacy and medical teams can provide effective patient care without shouldering the traditional risks of opioids.
Although suzetrigine has only been studied in acute pain treatment thus far, this medication is a significant step forward for pain management. Clinicians constantly juggle the pressing need to provide adequate pain relief against the severe risks of opioid adverse events. Journavx (suzetrigine) provides us with an effective option without the worry of sedation, respiratory depression, and addiction.
References
- Understanding the opioid overdose epidemic. Centers for Disease Control and Prevention. June 9, 2025. Accessed July 5, 2026. https://www.cdc.gov/overdose-prevention/about/understanding-the-opioid-overdose-epidemic.html
- JOURNAVX® (suzetrigine). Boston, MA: Vertex Pharmaceuticals. Accessed July 5, 2026. https://www.journavxhcp.com/
- Suzetrigine. Lexi-Drugs. UpToDate Lexidrug. UpToDate Inc. https://online.lexi.com. Accessed July 5, 2026.
- Nikitin, D., Rind, D. M., McQueen, B., Raymond, F., Sanchez, S., DiStefano, M. J., Zemplenyi, A., Lee, W., & Ollendorf, D. (2025). The effectiveness and value of suzetrigine for moderate to severe acute pain: A summary from the Institute for Clinical and Economic Review's Midwest Comparative Effectiveness Public Advisory Council. Journal of managed care & specialty pharmacy, 31(7), 729–734. https://doi.org/10.18553/jmcp.2025.31.7.729
- Bertoch, T., D'Aunno, D., McCoun, J., Solanki, D., Taber, L., Urban, J., Oswald, J., Swisher, M. W., Tian, S., Miao, X., Correll, D. J., Negulescu, P., Bozic, C., & Weiner, S. G. (2025). Suzetrigine, a Nonopioid Na V 1.8 Inhibitor for Treatment of Moderate-to-severe Acute Pain: Two Phase 3 Randomized Clinical Trials. Anesthesiology, 142(6), 1085–1099. https://doi.org/10.1097/ALN.0000000000005460
- McCoun, J., Winkle, P., Solanki, D., Urban, J., Bertoch, T., Oswald, J., Swisher, M. W., Taber, L. A., Healey, T., Jazic, I., Correll, D. J., Negulescu, P. A., Bozic, C., Weiner, S. G., & VX-548-107 Study Team (2025). Suzetrigine, a Non-Opioid NaV1.8 Inhibitor With Broad Applicability for Moderate-to-Severe Acute Pain: A Phase 3 Single-Arm Study for Surgical or Non-Surgical Acute Pain. Journal of pain research, 18, 1569–1576. https://doi.org/10.2147/JPR.S509144
*Information presented on RxTeach does not represent the opinion of any specific company, organization, or team other than the authors themselves. No patient-provider relationship is created.