
The Anti-Smoking Antidepressant
Bupropion’s dopamine and norepinephrine effects reduce nicotine cravings, explaining its FDA approval as a first-line smoking cessation aid now.


Author: Dylan Hembrough, PharmD Candidate Class of 2028
Editor: Kristen Linduaer, PharmD, BCPS, AAHIVP
Bupropion (Wellbutrin) stands among fluoxetine (Prozac) and sertraline (Zoloft) as one of the most well-known antidepressants.
So how did it get indicated for smoking cessation?
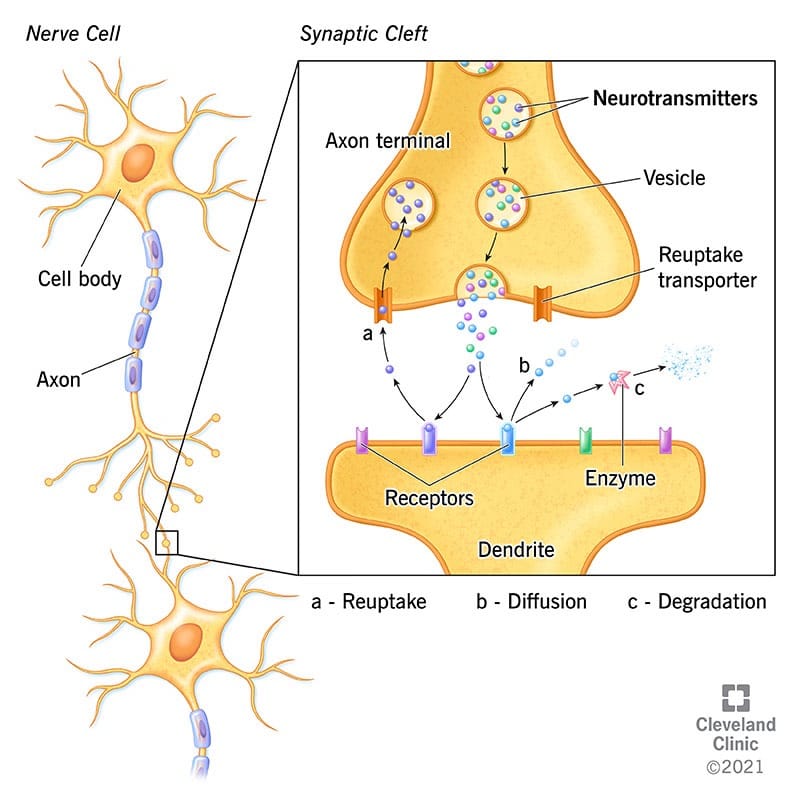
Bupropion is a norepinephrine-dopamine reuptake inhibitor. It works in the spaces between nerve cells, called synapses.1 When nerve signals are propagated, chemicals called neurotransmitters travel across the synapse to ignite the signal in the next neuron.1 After this, they are subject to “reuptake,” when the first neuron reabsorbs them for later use.1 See Figure 1 below for a visual representation of the mechanism of action of norepinephrine-dopamine reuptake inhibitors.
This mechanism of action is very similar to that of the larger selective serotonin reuptake inhibitor (SSRI) class. While drugs like fluoxetine and sertraline inhibit the reuptake of serotonin in the synaptic spaces, bupropion does the same with norepinephrine and dopamine.2 Because bupropion acts on norepinephrine and dopamine, it can be used either as a monotherapy or as an adjunct therapy with SSRIs.3
It is thought that the unique niche of bupropion in the brain lends to its anti-nicotine properties as well. Nicotine stimulates the release of a handful of neurotransmitters — dopamine among them.3 Dopamine in particular is an agent of the “reward pathway,” which induces pleasure and reinforces dependence and addiction.3 Bupropion mimics the effect of nicotine and diminishes the effect of nicotine on nicotine receptors, leading to decreased nicotine cravings.4
Bupropion was initially approved by the FDA in 1985, but was removed from the market the following year due to seizure concerns.3 It was reintroduced in 1989, but it didn’t pick up the smoking cessation indication until 1997.3 When it did, it became the first non-nicotine treatment option for nicotine addiction.4
In 1997, bupropion monotherapy demonstrated a smoking cessation rate of up to 23.1% one year after treatment, compared to a placebo rate of 12.4%.5 Without therapy, only around 5% of quit attempts are successful.6
These results were impressive enough to make sustained-release bupropion a first-line treatment option for nicotine addiction. Just like with depression, bupropion can be used alongside other nicotine addiction treatments in an effort to increase the likelihood of smoking cessation.
Many studies over the past two and a half decades have shown combination therapy to be quite effective in the short-term.
“The abstinence rates at 12 months were 15.6% in the placebo group, as compared with 16.4% in the nicotine-patch group, 30.3% in the bupropion group, and 35.5% in the group given bupropion and the nicotine patch,” a 1999 study determined.6
However, the long-term efficacy of bupropion beyond the duration of treatment referenced in the study above is less clear.
“Most of the large trials suggest that a positive benefit with bupropion therapy may be sustained up to one year, but the early success demonstrated by Zellwegger, et al. (2005) was not sustained following withdrawal of treatment,” one 2008 article said. “This supports the theory that bupropion does not modify neurotransmitter activity and has no longer-term effects beyond the treatment period.”4
Bupropion is sometimes prescribed in combination with other non-nicotine therapies, like varenicline (Chantix). However, the long-term efficacy of this combination therapy runs into the same issues as bupropion paired with nicotine replacement.7
Many studies also showed that the adverse effects of bupropion may be strong enough to warrant discontinuing therapy in some patients. Insomnia, nausea and vomiting, and dizziness were the most commonly reported, and bupropion is explicitly contraindicated in patients who experience seizures, though seizures are a very rare side effect overall.4
All that said, smoking cessation and nicotine addiction are just as psychological as they are physiological. This is particularly noteworthy when considering the effects of nicotine withdrawal, which often include anxiety and depression.7
What many of these studies lack is an analysis of the effect of cognitive behavioral therapy, for example, in the months after drug therapy. The main focus of these studies is on the efficacy of the drug, so the studies do what they set out to do. But there is more to nicotine addiction than drug efficacy, and the psychological aspect of addiction is a major player in patient outcomes.
Bupropion certainly has a place as a smoking cessation therapy, but for long-term abstinence and prevention of smoking relapse, it should next be studied as a part of the wider and much more complex nature of nicotine addiction.
If you or someone you know is interested in quitting smoking or nicotine products, consult your provider for treatment or call the smoking cessation hotline at 1-800-QUIT-NOW.
About the Author

References
1 Neurotransmitters. Cleveland Clinic. 2022 Mar 14.
2 Bupropion. Clinical Pharmacology.
3 Huecker MR, et al. Bupropion. National Institutes of Health. StatPearls Publishing LLC. 2024 Sep 2.
*Information presented on RxTeach does not represent the opinion of any specific company, organization, or team other than the authors themselves. No patient-provider relationship is created.