
DOACs for Venous Thromboembolism: Which is the Best?
A practical comparison of DOACs for VTE, covering indications, dosing, bleeding risk, renal considerations, and reversal.

Direct oral anticoagulants (DOACs) are blood thinning medications meant to decrease the chance of thrombotic events like strokes or deep vein thrombosis.1 There are currently four DOACs on the market, three of which are factor Xa inhibitors, and one of which is a direct thrombin inhibitor.1
All factor Xa inhibitors work the same way. In the convoluted process that is the clotting cascade (Figure 1), factor Xa serves a “gatekeeper” function – it is the first clotting factor required by both arms of the cascade to proceed.2 Thus, inhibiting factor Xa stops the clotting cascade altogether.
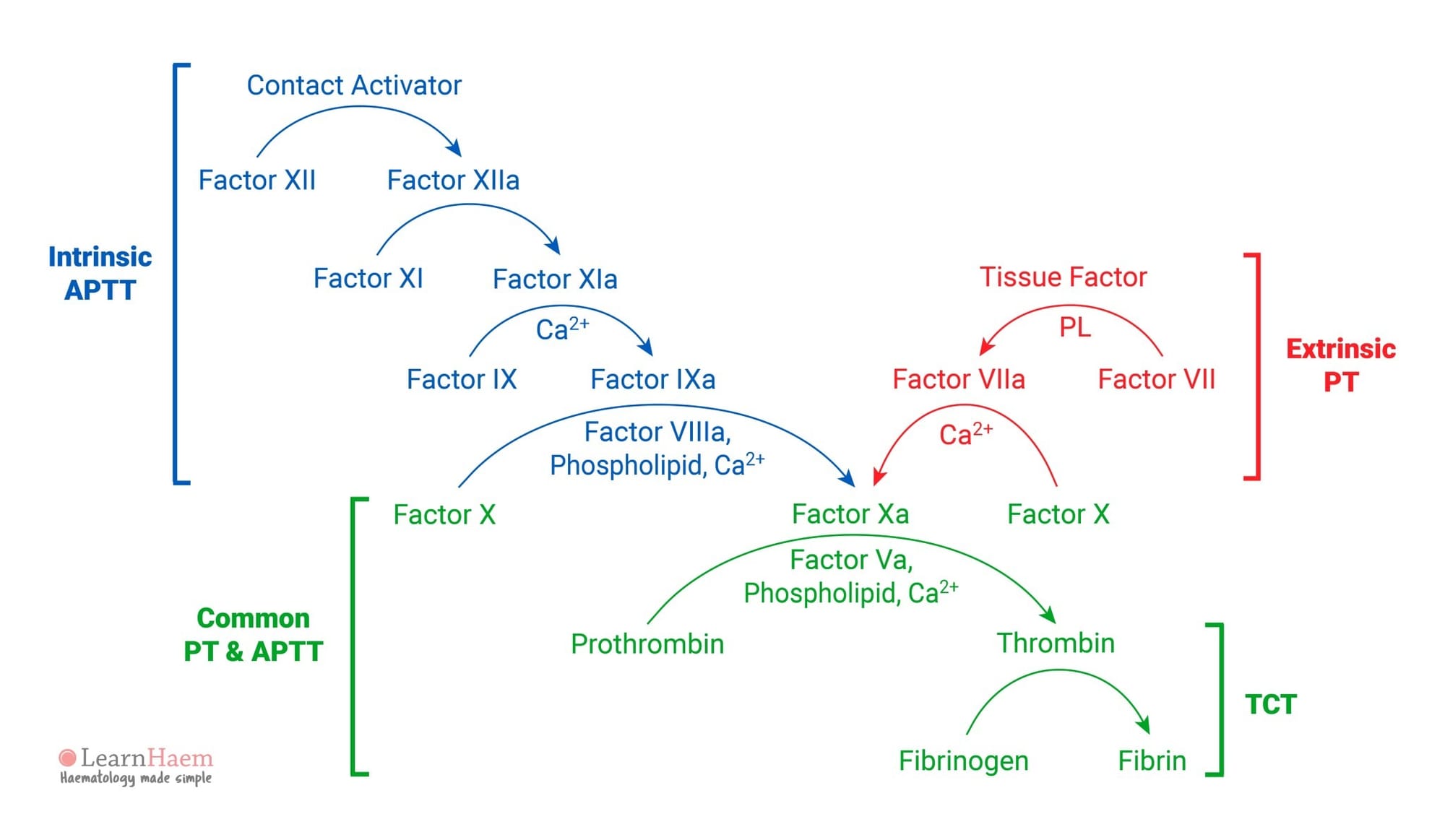
Direct thrombin inhibitors, on the other hand, block the action of thrombin. Thrombin is immediately downstream of factor Xa in the clotting cascade and is responsible for activating fibrin, the main component of blood clots.2 Thrombin also triggers platelet aggregation as well – in other words, it makes platelets start to gather at the site of the future clot.3
For more information on periprocedural management and transitioning between DOACs, check out our article on these concepts here.

So, how do these drugs stack up against each other?
Abbreviations used in the following sections
PO = oral or by mouth
BID = twice daily dosing
VTE = venous thromboembolism
Apixaban (Eliquis)
Apixaban is a factor Xa inhibitor and received FDA approval in 2012.4 Apixaban is indicated for both venous thromboembolism prophylaxis and treatment.5 Dosing for prophylaxis is 2.5 mg PO BID and for treatment is 10 mg PO BID for 7 days, followed by 5 mg PO BID.5 Apixaban can be taken at any time without regard to meals.
As with all blood thinners, abnormal bleeding is an unsurprising adverse effect, and ≤15% of adults experience this while taking apixaban.5 While factor Xa inhibitors historically have been considered equal in bleed risk, a March 2026 study comparing apixaban and rivaroxaban (Xarelto) demonstrated that apixaban has a lower bleed risk than rivaroxaban.6 Other than that, apixaban is generally well-tolerated. Routine coagulation testing is not necessary.5
Apixaban has not been studied in patients with a creatinine clearance (CrCl) of <25 mL/min.5 While the manufacturer says no dose adjustment is necessary, there is very limited data available for the use of apixaban in renally-impaired patients.5 Thus, apixaban is generally avoided in patients with renal impairment.5
Apixaban is also minimally dialyzable.5 Again, according to the prescribing information (also noted in LexiComp), the manufacturer maintains that no dose adjustment is necessary, but objective data is still severely limited.5
In hepatic impairment, apixaban can be used safely in patients with a baseline Child-Pugh class A or B for venous thromboembolism prophylaxis and treatment.5 Baseline class C patients, however, should not receive apixaban for treatment.5 A patient who progresses to class C from a different baseline should be switched to another anticoagulant.5 Since prophylaxis and indefinite coagulation therapy are dosed lower, there is some debate over the safety of apixaban in class C patients, but some guidelines still recommend against apixaban use.5
Apixaban is metabolized by CYP3A4, so strong inducers or inhibitors of that enzyme interact heavily with apixaban and are to be avoided or very closely monitored.5 Apixaban is contraindicated with dual CYP3A4 and P-gp inducers.5
There is a boxed warning for spinal or epidural hematoma for patients undergoing spinal puncture or receiving neuraxial anesthesia.5 There is also a boxed warning for premature discontinuation of therapy and the increased risk of thrombotic events.5
Apixaban has not been studied in pregnant populations, and the use of apixaban for this population is avoided.5
Rivaroxaban (Xarelto)
Rivaroxaban is a factor Xa inhibitor that received FDA approval in 2011.7 Rivaroxaban is dosed at 10 mg PO daily for VTE prophylaxis, and for treatment at 15 mg PO BID for 21 days followed by 20 mg PO daily with food.8
Rivaroxaban is associated with much higher bleed risk than apixaban.6 According to LexiComp, anywhere from 5-36% of adult patients experience hemorrhaging while taking rivaroxaban.8 Routine coagulation testing is not necessary.8
The use of rivaroxaban in renal impairment is even more restricted, with a CrCl of ≤30 mL/min being an absolute contraindication to use.8 Rivaroxaban is not dialyzable and cannot be used in patients receiving hemodialysis.8
The use of rivaroxaban in liver impairment is also more restricted. No dose adjustment is necessary for patients in Child-Pugh class A, but use is not recommended (or at least strongly discouraged) in classes B and C.8
Like apixaban, rivaroxaban interacts strongly with strong CYP3A4 inducers and inhibitors, and rivaroxaban should not be used concomitantly with dual CYP3A4 and P-gp inducers.8
Rivaroxaban has the same boxed warnings as apixaban and is avoided in pregnant populations as well.8
Edoxaban (Savaysa)
Edoxaban is also a factor Xa inhibitor and was approved by the FDA in 2015.9 Edoxaban has a similar profile to apixaban and rivaroxaban, but the use of edoxaban is much more limited. Edoxaban is not indicated for VTE prophylaxis, and edoxaban is not an initial treatment option either.10 Only after 5 days of treatment with a parenteral anticoagulant does edoxaban become an option for maintenance therapy.10
If used, edoxaban is dosed at 60 mg PO daily for patients >60 kg and 30 mg PO daily for patients <60 kg.10
Hemorrhage (7-26%) and major hemorrhage (1-13%) are significant adverse effects of edoxaban.10 Routine coagulation testing is not necessary.10
Edoxaban is not significantly dialyzable and is contraindicated in CrCl ≤15 mL/min.10 Interestingly, edoxaban is also generally recommended against in CrCl >95 mL/min due to an increased risk of recurrent VTE – increased renal clearance results in less drug in the body.10 Limited data suggests a dose of 30 mg PO daily is safe in patients between a CrCl of 15 and 50 mL/min.10
Use is not recommended in patients with Child-Pugh class B or C.10
Edoxaban is not metabolized by CYP3A4 and does not interact with inducers or inhibitors of that enzyme.10 However, edoxaban is a substrate of P-gp and should be avoided with P-gp inducers and very closely monitored, if not avoided, with P-gp inhibitors.10
In addition to the previous two boxed warnings, edoxaban has a third warning for reduced efficacy in patients with nonvalvular atrial fibrillation and a CrCl >95 mL/min.10 Edoxaban is also avoided in pregnant populations.10
Dabigatran (Pradaxa)
Dabigatran, a direct thrombin inhibitor, is a prodrug and is the earliest of the DOACs to come to market, having been approved by the FDA in 2010.11,12 It is only used for VTE prophylaxis after a total hip arthroplasty or total knee arthroplasty (off-label).12 Like edoxaban, dabigatran is not an initial option for VTE treatment and must follow an initial 5 days of parenteral anticoagulation.12 In this setting, dabigatran is dosed at 150 mg PO BID.
Dabigatran is well-known among the DOACs for gastrointestinal side effects. 25-40% of patients receiving dabigatran experience gastrointestinal upset, according to LexiComp.12 Hemorrhage also occurs in 10-19% of patients.12
Dabigatran cannot be used in patients with a CrCl of <30 mL/min, regardless of prophylaxis or treatment.12 Dabigatran is dialyzable, but use is still avoided in patients receiving hemodialysis.12
What dabigatran does have over the factor Xa inhibitors is that hepatic impairment has no effect on dosing.12
Dabigatran is a substrate of P-gp and should be avoided concomitantly with P-gp inducers.12 Use with P-gp inhibitors should be closely monitored.12
Dabigatran can be reversed in the scenario of an overdose where severe bleeding is occurring. This is accomplished with idarucizumab (Praxbind).13 However, being a monoclonal antibody, idarucizumab is very costly. Prothrombin complex concentrate (PCC) is also an option for reversal, but it is less effective than idarucizumab.16
Factor Xa inhibitors must rely on PCC for reversal, which is technically an off-label indication.14 Andexanet alfa (Andexxa) was a dedicated reversal option briefly, but it was pulled from the market last year after new post-marketing safety data came to light.14
Dabigatran is not recommended in pregnant populations.12 Dabigatran has the same two boxed warnings as apixaban and rivaroxaban.12
Conclusions
The factor Xa inhibitors are, by and large, an impressive class of drugs. Apixaban seems to be the best option overall, a convenient and reliable choice for VTE prophylaxis and treatment. If factor Xa inhibitors are not an option, such as in those with severe hepatic impairment, dabigatran serves as a decent alternative.
A weakness of the DOACs is the inability to use them in settings of renal impairment. For these patients, the much older agent warfarin (Coumadin) may be the best option.
The DOACs also cannot be used in pregnant patients – unfractionated heparin and low-molecular weight heparin are the preferred agents in this population.17 And, being anticoagulants, the DOACs all carry with them the risk of abnormal bleeding. However, this risk is easier to manage than the wildly variable bleed risk presented by warfarin. The extent of anticoagulation does not need to be routinely monitored either, since all DOACs have a relatively reliable effect.
DOACs have been around for a relatively short time, but are already among the most widely-used drugs in their field: a testament to their efficacy and relative reliability.
LexiComp offers a convenient chart for quickly comparing the DOACs to each other and with warfarin.15
References
- Chen A, Stecker E, Warden BA. Direct Oral Anticoagulant Use: A Practical Guide to Common Clinical Challenges. Journal of the American Heart Association. 2020 Jun 15;9(13).
- The Revised Coagulation Cascade. LearnHaem. 2020 Aug 17.
- Comin J, Kallmes DF. Dabigatran (Pradaxa). AJNR Am J Neuroradiol. 2012 Mar;33(3):426-428.
- Eliquis FDA Approval History. Drugs.com.
- Apixaban. Lexidrug.
- Castellucci LA, et al. Bleeding Risk with Apixaban vs. Rivaroxaban in Acute Venous Thromboembolism. N Engl J Med 2026 Mar 11;394:1051-1060.
- Stewart J. Xarelto FDA Approval History. Drugs.com. 2021 Dec 26.
- Rivaroxaban. Lexidrug.
- Savaysa FDA Approval History. Drugs.com.
- Edoxaban. Lexidrug.
- Stewart J. Pradaxa FDA Approval History. Drugs.com. 2021 Jun 28.
- Dabigatran Etexilate. Lexidrug.
- Giannandrea D, et al. Practical considerations on anticoagulation reversal: spotlight on the reversal of dabigatran. Vasc Health Risk Manag. 2019 May 23;15:139-142.
- Jobe R. The Andexxa Paradox. RxTeach. 2026 Jan 14.
- Oral Anticoagulant Comparison Chart. Lexidrug.
- Reversing the Blood-Thinning Effects of Dabigatran: Idarucizumab Versus Prothrombin Complex Concentrates. American Society of Hematology.
- Zaidi SRH, Jenkins SM. Anticoagulant Therapy In Pregnancy. National Institutes of Health. StatPearls Publishing LLC. 2024 Jan 10.
*Information presented on RxTeach does not represent the opinion of any specific company, organization, or team other than the authors themselves. No patient-provider relationship is created.